Bispecifics Have Cleared the First Hurdle
The Next Is Scale
Authored by Ronald Deng; Shana Gunderson Hua, PharmD
What you’ll learn:
Oncology bispecifics are entering a scale-up phase in which the constraint is no longer proof of concept, but whether the market can absorb them.
As solid tumors and flexible delivery models emerge, adoption will be shaped by care-setting fit, treatment burden, and stakeholder confidence as much as efficacy.
The next commercial advantage will come from designing therapies not just to work but to scale across the oncology ecosystem.
Bispecific antibodies have rapidly emerged as one of oncology’s most commercially significant immunotherapy modalities. By binding both a tumor cell and a T-cell simultaneously, these engineered therapies bring immune effector cells into close proximity with cancer cells, helping overcome the immune-evasion mechanisms that often limit traditional approaches.
The clinical significance of bispecifics lies in combining the accessibility of a standard drug (off-the-shelf, no patient-specific manufacturing) with efficacy that rivals far more complex therapies like CAR-T. Approved agents have already demonstrated strong responses in patients who had exhausted other options, and the modality is rapidly expanding from blood cancers into solid tumors.
For the past several years, the industry has focused on clinical proof of concept and safe administration. Management of cytokine release syndrome, step-up dosing, and site-of-care protocols have defined the conversation. While these remain essential, they are no longer enough to set a therapy apart. As more bispecifics clear the initial bar for efficacy and manageability, differentiation is shifting to a harder question: which therapies can scale across real-world care settings, reimbursement pathways, and stakeholder workflows.
Bispecifics are no longer competing solely on science. They are competing on how easily the market can absorb them.
Where the Next Bottleneck Is Emerging
The move from scientific validation to real-world adoption is happening just as the category itself is expanding. The next wave is now emerging on two fronts simultaneously: expansion into solid tumors and greater flexibility in how these therapies are delivered.
Each introduces a new layer of commercial complexity. Solid-tumor expansion multiplies the number of payer, diagnostic, and treatment-site variables a therapy has to work through. Delivery flexibility asks brands to work in care settings they were never built for.
FROM THE WORK
For bispecifics to scale in real-world oncology, evidence, access, delivery, and stakeholder behavior have to move as one connected system. Treating them separately is where launch friction begins. In practice, evidence, access, delivery, and stakeholder behavior have to move together. Treating them as separate workstreams is where launch friction begins.
Recent approvals make the inflection point visible. Tarlatamab’s traditional FDA approval in extensive-stage small cell lung cancer confirms that solid-tumor validation is no longer theoretical.[1] At the same time, subcutaneous amivantamab signals that delivery innovation is becoming commercially meaningful, reducing the administrative burden and treatment friction in ways that can influence real-world adoption.[2]
The next constraint in bispecifics is not awareness. It is not even access in the traditional sense. It is adoption friction across the oncology ecosystem.
Payers are looking beyond efficacy to total cost-of-care. Providers are navigating more complex sequencing, safety, and workflow realities. Community oncology sites are asking whether these therapies can be delivered outside specialized centers. Patients and caregivers are absorbing the cumulative burden of monitoring, travel, waiting, and uncertainty.[3,4,5]
These pressures do not operate independently, they compound.
FROM THE WORK
We recently modeled reimbursement risk for a bispecific across treatment sites, using more than 10,000 scenarios that accounted for clinical context, dosing, acquisition channel, coding and billing mechanics, and payer dynamics.
The analysis showed that risk was not concentrated in an independent variable but modified based on specific interactions. Dose-level waste, site-specific billing rules, diagnostic coverage, and patient continuation all influenced the economic picture.
For bispecifics, that is the practical commercialization challenge: reimbursement risk has to be modelled across real-world conditions as every scenario is different.
The Four Fits of Bispecific Scale
In this next phase, every bispecific will face four tests. Failure in any one of them will slow adoption.
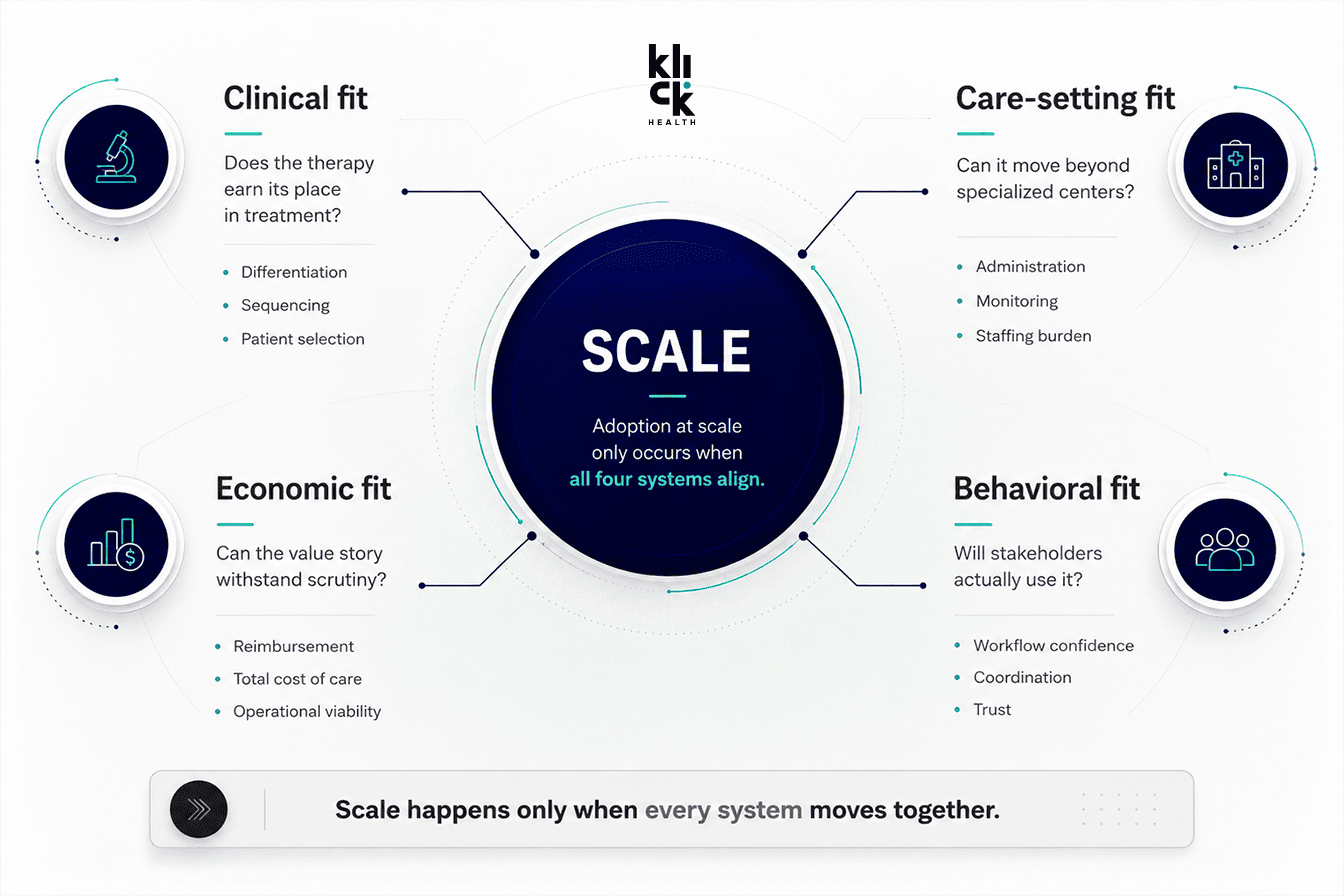
Figure: The Four Fits bispecifics have to pass to scale.
1. Clinical fit
Does the therapy earn its place in treatment? Clinical differentiation is necessary, but no longer decisive on its own.
In practice: When two bispecifics appear similar in trial data, the therapy with the clearer sequencing story and patient-selection rationale is easier for providers, payers, and care teams to act on.
2. Care-setting fit
Can it move beyond specialized centers into broader practice? Administration complexity, monitoring requirements, and staffing burden now determine whether therapies can expand into community oncology.
In practice: Sites of care sit on a readiness spectrum. Some can absorb complexity and build capability over time. Others need a launch model that is simple, supported, and operationally clear from day one. A strategy built for one end of that spectrum will stall at the other. Scaling requires knowing which sites are ready now, which need support, and where friction will limit uptake.
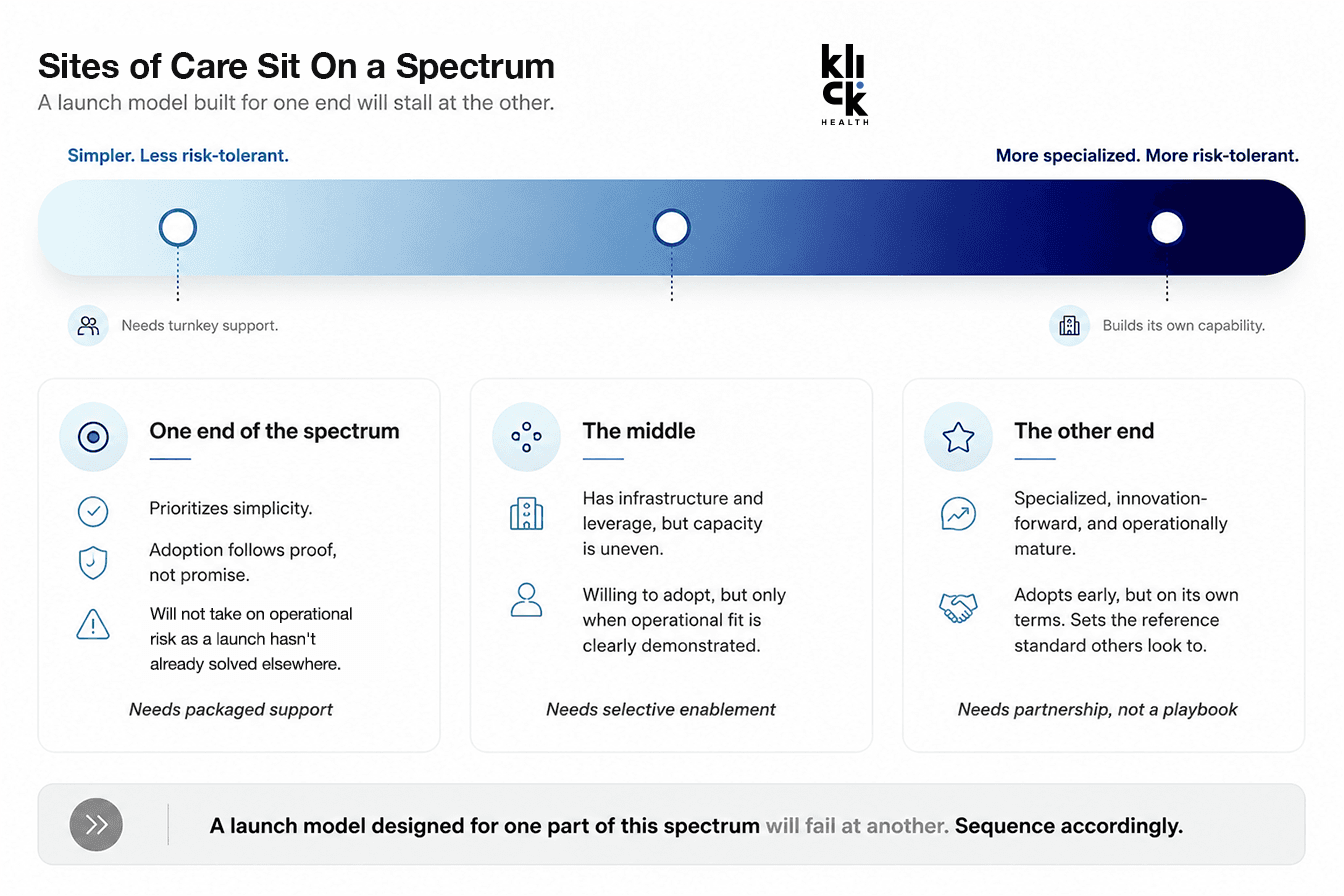
Figure: Sites of Care on a spectrum and what each end needs from a launch.
3. Economic fit
Can the value story hold up in the real world? Payers and health systems are looking beyond drug cost to the full cost of care, including site of care, resource use, billing complexity, and reimbursement risk.
In practice: Reimbursement risk is not static. It changes by dose, site of care, payer, and acquisition model. Early doses may carry more waste or inpatient exposure, while later doses may reimburse differently. 340B status can change the economics again. Economic fit has to be modeled across those variables.
4. Behavioral fit
Will stakeholders actually use it? Adoption depends on whether providers, care teams, and patients can confidently integrate the therapy into real-world workflows.
In practice: Behavioral fit occurs when medical education, field enablement, and patient experience either reinforce or work against each other. When touch points are designed as a single system, the therapy feels coordinated for the people being asked to start it. That confidence is what moves adoption.
The Four fFts are not parallel considerations. They are interdependent constraints. Scale happens only when all four conditions are met simultaneously.
Delivery Design Is Becoming Brand Strategy
What is changing, and often underestimated, is that decisions once considered purely scientific are now shaping commercial outcomes. Subcutaneous administration, simplified dosing, and reduced administration-related reactions are more than incremental improvements. They determine whether a therapy can move into lower-intensity care settings, reduce staffing constraints, and lower the perceived risk of adoption.
The FDA’s decision on amivantamab, supported by data showing significantly fewer administration-related reactions with subcutaneous delivery, is an early signal of how deployability can become a competitive differentiator.[2]
This dynamic extends beyond administration. The concept of “time toxicity” has reframed oncology-treatment burden around the cumulative time patients spend interacting with the healthcare system.[3] A JAMA Network open study of more than 55,000 patients with metastatic cancer found 40.1 to 62.9 healthcare contact days in the year following diagnosis.[4] While not specific to bispecifics, the implication is increasingly relevant: treatment burden is becoming more visible, more measurable, and more commercially meaningful.
CAR-T provides the closest analog. Expanding CAR-T into outpatient settings required far more than a manageable safety profile. It required infrastructure, coordination, reimbursement alignment, and sustained education.[5] Bispecifics are now approaching a similar threshold.

What “At Scale” Actually Means
The question is no longer whether these therapies can be delivered, it is whether they can be delivered at scale across the environments where most patients receive care.
For biopharma, this exposes a structural problem. Traditional launch models are not built for this level of interdependence. Market access, medical, analytics, and brand still operate too often as parallel workstreams, each optimizing for its own objectives. But adoption does not happen in silos.
It happens at the intersections where value narratives align with clinical positioning. Where medical education supports real-world delivery. Where account strategy reflects operational readiness. Where patient experience aligns with the realities of access and reimbursement.
Fragmentation creates friction. Alignment reduces it.
This is orchestration as strategy. When access depends on delivery, delivery depends on education, education depends on confidence, and confidence depends on how clearly the science is explained, the model itself becomes the constraint.
FROM THE WORK
Passing all four fits requires market access, medical, regulatory, brand, creative, and technology teams to work as one system.
That is where Klick’s model matters. By bringing value strategy, evidence translation, care-setting readiness, stakeholder education, and customer experience together, handoffs between functions become invisible to the market. The result are therapies that are easier for payers, providers, sites of care, and patients to absorb.
The opportunity ahead is significant. Bispecifics will continue to expand into solid tumors.[1] Delivery models will keep evolving.[2] Competitive density will increase. Health systems will face growing pressure on cost, complexity, and capacity. Incremental improvements won’t be enough in that environment.
The next leaders in bispecifics will not be the ones with the most interesting molecule. They will be the ones who make complex innovation easiest for the market to absorb.
Bispecifics have cleared the first hurdle. The next is scale.

References
FDA grants traditional approval to tarlatamab-dlle for extensive-stage small cell lung cancer. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-traditional-approval-tarlatamab-dlle-extensive-stage-small-cell-lung-cancer
FDA approves amivantamab and hyaluronidase-lpuj for subcutaneous injection. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-amivantamab-and-hyaluronidase-lpuj-subcutaneous-injection
The Time Toxicity of Cancer Treatment (Journal of Clinical Oncology). https://ascopubs.org/doi/pdfdirect/10.1200/JCO.21.02810
Health Care Contact Days in Older Adults with Metastatic Cancer (JAMA Network Open). https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2842561
Outpatient CAR T-Cell Therapy as Standard of Care: Current Perspectives and Considerations. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11086991/
Klick Health is the world’s largest independent commercialization partner for life sciences and a leading full-service pharma marketing partner, serving as agency of record for leading pharma, biotech, and healthcare brands. Klick’s specialized offerings are rooted in deep medical and scientific understanding, including market insights, award-winning creative, and proprietary AI and data models to craft impactful brand narratives and seamless customer journeys. Backed by nearly 250 medical experts and advanced healthcare analytics, Klick delivers integrated marketing strategy and communications, from new product launch strategy to MLR review with real-world evidence, helping brands thrive in today’s complex healthcare landscape. Learn more at Klick.com.
Authors

Ronald Deng
VP, Content Expert, Market Access

Shana Gunderson Hua, PharmD
SVP, Market Access Strategy

Ready to Drive Life Sciences Forward?
Experience the transformative power of Klick Health, where deep industry expertise meets cutting-edge AI-driven wisdom.
As your trusted partners in life sciences commercialization, we combine a storied history in healthcare with the latest technologies to elevate every facet of your omnichannel strategy. From crafting engaging narratives to enabling data-driven decision-making, our integrated capabilities ensure you lead the way in transforming patient outcomes through digital health innovation.
Let’s create something transformative together.
